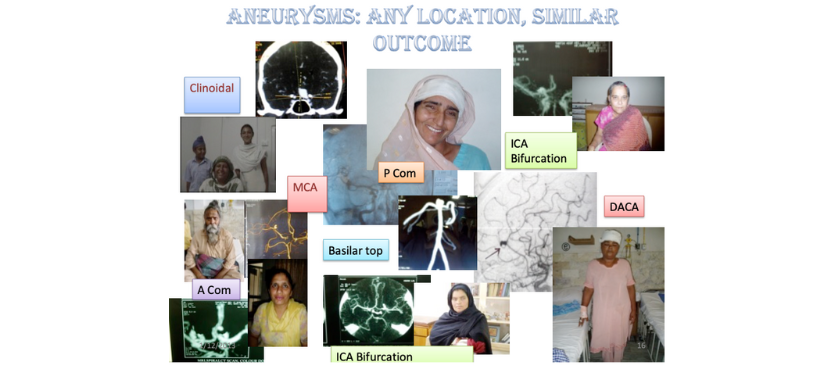
Our treatment options include.
We operate all grade (even grade 4-5) aneurysms, at any time after bleed,irrespective of status of vasospasm, at the earliest possible time. We generally do not use temporary clipping, thus avoid ischemia. For last many cases we do not use any retractor on brain or minimal retraction only.
We have been doing about 15-25 cases every year, No intra-operative death in 13 years experience. Postop death due to vasospasm in 5-10% cases. Last year we did not have any mortality out of 21 surgeries. Almost all cases operated have been in follow up and none had any rebleed after surgery.
A case with large ICH with brainstem herniation was operated even without angiography and was saved.
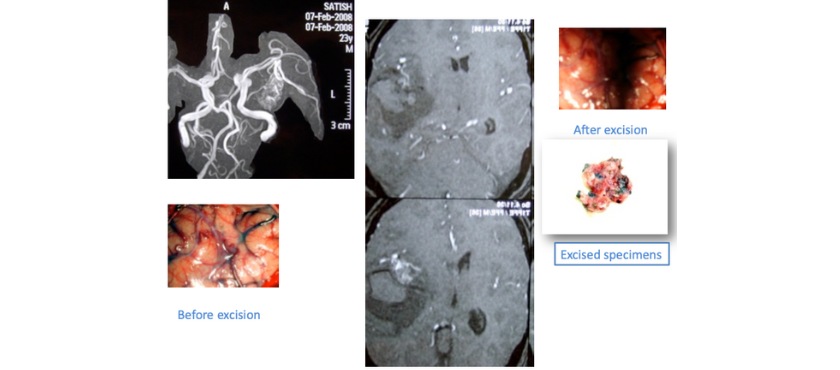
Case of AVM with specimen
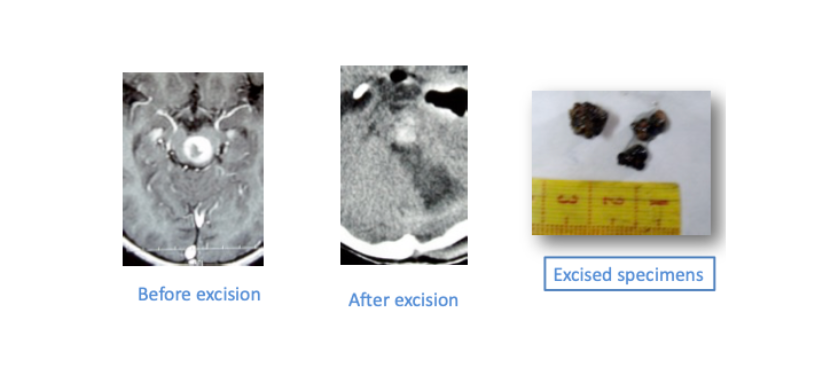
Case of brainstem cavernoma excised with endoscope by suboccipital Supracerebellar approach
Microsurgical decompression with or without stereotactic localization with trans-sulcal approach or small (1 cm) corticectomy in certain cases may expedite the recovery process, may restore the focal deficits (hemiparesis etc), may decrease hospital stay and decrease the need of diuretic/mannitol etc (thus decreases the risk to kidney function in elderly). Surgery safely done in as old as 75-80 years at our hospital.
The centre is known for minimally invasive / Key-hole Endoscopic and Microsurgical Spine and Brain surgery. The senior spine and neurosurgeon has more than 18 years experience with endoscopic techniques
© 2023 HMC Hospital, All Rights Reserved.
Made with ❤️ By Digital Darzee